Microlaryngoscopy and Surgery to the Vocal Folds
Microlaryngoscopy is an examination of the larynx under a general anaesthetic using magnification. Sometimes it is done purely for diagnostic purposes, but more commonly it is to carry out very fine microsurgery on the vocal cords using fine instruments.
 A microlaryngoscopy – the laryngoscope is suspended through a patients mouth(not shown) allowing work with fine instruments under magnification.
A microlaryngoscopy – the laryngoscope is suspended through a patients mouth(not shown) allowing work with fine instruments under magnification.
Occasionally laser is used through the microscope which will require special anaesthetic technique
In most cases the procedure is done because of a change in voice.
The operation is usually straightforward. In a great majority of case it is done as a day case and you should be able to go home afterwards. However note that you will not be able to drive for 24 hours and you should have somebody accompanying you to the hospital.
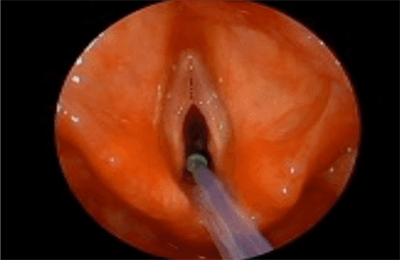
Operative view of the vocal cords at microlaryngoscopy
What are the Risks of the Procedure?
Operative view of the vocal cords at microlaryngoscopy
Like any operation there are risks associated with it, although the risks of the operation itself are only slight and seldom serious. Note that there are,of course,slight risks associated with a general anaesthetic and you should discuss these with the anaesthetist before the procedure.
The risks associated with the microlaryngoscopy itself are:
- Damage to teeth. Although all precautions are taken in shielding the teeth and using guards, nonetheless this can still sometimes occur. These are seldom gross injuries but more commonly slight chipping of the edge. When recognised we usually use a small diamond burr to grind this down so that they do not feel rough, but rarely you may need dental attention afterwards.
- Cuts and contusions of the mouth and throat and tongue. These can occur, although seldom. They can be painful for a few days.
- Inhalation of blood or pieces of the patients own tissue causing lung problems. This is theoretically possible but extremely rare.
- Jaw dislocation. This is very rare but theoretically possible.
- Laser burns. This can occur in those few cases where a laser is used. All precautions are takenagainst this, although theoretically it is possible.
- Sometimes there is a sensation of numbness of the tongue with altered taste. This usually subsides in a week or two.
- Bleeding. Very rarely significant unless you are on blood thinning agents such as Warfarin or Aspirin. If prolonged this is potentially hazardous to the airway. These agents should be ceased before an operation. Please discuss with your surgeon or GP
- Airway obstruction. Although theoretically always a risk, due to swelling or bleeding, when we operate on part of the upper airway (which the vocal folds are), in practice,this is very rare. If it did occur it might require some time with a tube in the larynx or a tracheostomy.
Please note that patients vary enormously in the ease with which their larynx may be visualised. This is why some people may also be difficult to give a general anaesthetic using an endotracheal tube. Some people are extremely easy to visualise using these techniques, whereas other people are almost impossible and there are all variations in-between. Anaesthetists actually use a grading system 1 -4 to express this. This is no reflection on the patient, but is a manifestation of particularfactors such as the presence and size of teeth and the configuration of the jaw and the ability to open the jaw, etc. Sometimes it is possible to predict this beforehand but by no means invariably so. If you have had a history of difficult intubation with a general anaesthetic then probably itwill be difficult to visualise you by this technique, although not necessarily impossible.
Post-Operatively
You will be taken back to the post-operative ward and then allowed to go home after two or three hours when fully conscious. Sometimes the procedure is combined with an oesophagoscopy in which case you will be kept for longer than normally for a microlaryngoscopy alone, and also you will not be able to eat for several hours.
After microlaryngoscopy alone however, you will be able to eat and drink very soon after the procedure.
You may spit up a little blood but this should not be a problemBreathing or wheezing should not be a problem but if you do experience them we do want to know about it.
Please note in the majority of cases where vocal cord surgery has been done you should not speak (at all!) for 3 days after the procedure.When you resume.
speaking please be a bit restrained for a week or two and avoid shouting, prolonged talking etc. Preferably you should follow your Speech Pathologists advice. Breathing should not be a problem.If you do experience problems we do want to know about it.
Why should I see a Speech Pathologist?
Most people would expect to see a physiotherapist after,say, surgeryto the knee or hip. We are dealing with much smaller,finer muscles in and around the larynx and in the same way the Speech Pathologist will give you exercises for these, to develop their functioning to optimal levels. Many will have already have had voice therapy prior to the operation. Youwill usually asked to make an appointment to see the Speech Pathologistwithin 10 to 14days of surgery. It is best if you book this before your surgery.
Mostly this will be with one of our Speech Pathologists here at MVAC . If there are geographical or time problems we can recommend a few in other centres but note that it must be with a Speech Pathologist with a special interest and expertise in voice-like doctors,Speech Pathologists do specialise.
After discharge,you will probably be asked to make an appointment to see the surgeon about two to four weeks later, preferably at MVAC,but sometimes at our ENT consulting rooms.
Important!
If you have any questions prior to the procedure please contact MVAC on 9416 0633.
If one is not contactable in an emergency,ring the other’s rooms. In an emergency after hours,ring the hospital where the surgery was done or Monash Medical Centre on 9495 6666 and ask to speak to the ENT registrar on duty.