Information for Retrograde Cricopharyngeal Muscle Dysfunction (R-CPD)
Definition:
Swallowing is a complicated sequence of both voluntary and reflex movements, which needs your brain to coordinate many muscles and nerves.
Dysphagia is the medical term for a sensation of difficulty or abnormality of swallowing. It can happen rapidly, or slowly and has many causes.
The cricopharyngeal (CP) muscle is the major component of the upper oesophageal sphincter, (UOS). It is a 1-2 cm wide, ring-like muscle that is normally constantly contracted, like a valve at the top of the oesophagus, except during swallowing. SEE Fig. 1. It physically sits in the lower midline neck. The other components of the UOS include the lower pharyngeal muscles, and the upper oesophageal muscles.
The cricopharyngeal (CP) muscle is involved in a number of finely controlled reflexes that control the passage of liquids, solids and gases down the oesophagus towards the stomach (anterograde movement), or up the oesophagus towards the mouth (retrograde). It usually either opens appropriately (e.g. Swallowing, Burping, vomiting) or tightens appropriately (e.g. Oesophageal reflux)
- Anterograde Reflexes: Swallowing
- Retrograde Reflexes: Burping, Vomiting, Reflux
Retrograde Cricopharyngeal dysfunction (R-CPD) is thus a condition in which the retrograde burp reflex doesn’t occur at all, or only very rarely, leading to a build-up of gas in the oesophagus and digestive tract, and a constellation of often very debilitating symptoms (see below).
The condition is generally non-progressive, but also non-resolving, meaning that, untreated, the condition remains with you, but won’t lead to increasing severity or further complications such as cancer, or an inability to swallow.
This condition was first formally described in the medical literature in 2018, and since then there have been increasing studies published regarding its causes, diagnosis, and treatment.
Causes:
There is no identified underlying cause for this condition.
R-CPD is a ‘functional’ condition, meaning, that whilst the CP muscle looks normal and identical to the muscle in patients without the condition, and functions appropriately for all other reflexes, it doesn’t function appropriately for the burp reflex (and occasionally the vomiting reflex as well).
Conditions that may mimic or co-exist with R-CPD include: Oesophageal Reflux, Eosinophilic Oesophagitis, SIBO, gastric inlet patch
Diagnosis:
The diagnosis of R-CPD involves a thorough case history, and a clinical examination of the muscles and nerves required for swallowing, and digital nasendoscopy of the upper airway and pharynx.
| 4 Key Symptoms |
| 1. The inability belch / burp |
| 2. Abdominal bloating and discomfort/nausea, or chest pain, especially after eating |
| 3. Socially awkward gurgling noises from the chest and lower neck as though the oesophagus is churning and straining to eject the air |
| 4. Excessive flatulence |
| Other Associated Symptoms |
| 1. Painful hiccups |
| 2. nausea |
| 3. Excessive saliva in response to the need to burp |
| 4. Shortness of breath with exertion due to inability to inhale fully due to oesophageal / abdominal air |
| 5. Significant impact on quality of life and social inhibition due to above symptoms |
However, unlike swallowing disorders, it does not necessarily require additional tests for diagnosis, unless there are symptoms in your history that are not typical for R-CPD, such as difficulty swallowing (dysphagia), disordered bowels habits, or unexplained weight loss.
Additional tests that sometimes may be required when there are non-typical symptoms include a standard barium swallow, video-stroboscopy, high resolution impedance manometry, pH testing and/or salivary pepsin testing. Often, a validated questionnaire, called a patient-related outcome measure, is often completed initially, and repeated later on to measure your progress. E.g. Eat-10 or SWAL-QOL.

Fig. 1 – Abdominal XR of a patient with R-CPD and gaseous abdominal bloating
Management:
Once you have had a consultation with the ENT surgeon and/or swallowing team you will generally fit into one of the following categories: Unlikely R-CPD, Possible R-CPD, and Probable R-CPD. If you have possible or probable R-CPD then on of the R-CPD treatment options will likely be advised. If it is unlikely that you have R-CPD, or possible, but with other atypical symptoms, then further tests and evaluations may be recommended first.
- Procedural/Surgical Treatments: (See Fig 2)
- Botulinum Toxin (Botox®) injection: Botox temporarily paralyses the muscle fibres in the CP, and possibly also effects the sensory nerve fibres, allowing better relaxation and stretching, and after 3 days, resumption of the burp reflex, and symptom resolution.
- Whilst the botox weakening only lasts for approximately 3 months, the benefits continue in most patients long-term
- This injection can be performed through the mouth (endoscopic), or through the neck (percutaneous).
- The Endoscopic route requires a general anaesthetic (asleep & unaware)
- At the same time your surgeon will evaluate your CP muscle and oesoaphagus for other possible causes (see above) and potentially take a biopsy (a small tissue sample) of any area of abnormality.
- The standard dose of Botox via this route is 75-100 Units, injected into the back ½ of the circular CP muscle
- The Percutaneous route requires local anaesthetic.
- EMG (electrical signal) guidance is used to precisely target the CP muscle from either side of the neck.
- A lower dose of botox is usually used via this route, 50-75 Units.
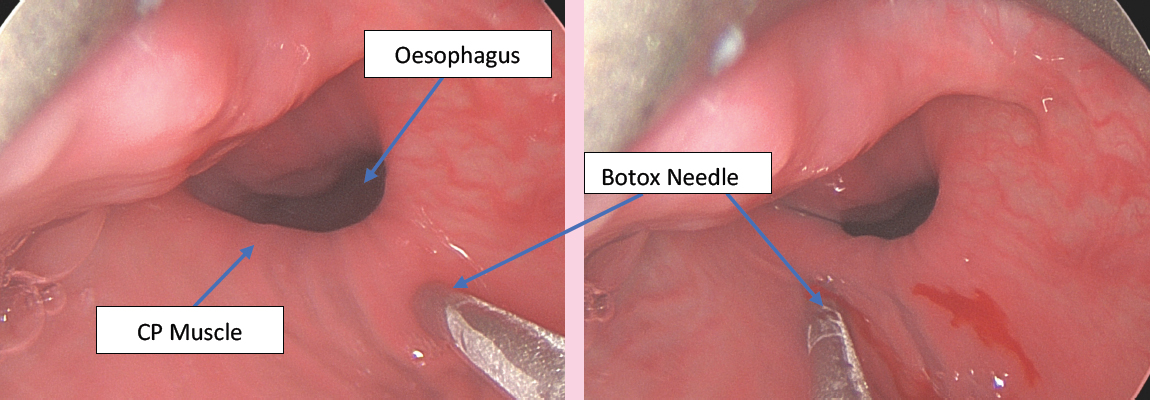
Fig. 2 – Multiple endoscopic injections of Botox® into back ½ of circular cricopharyngeal muscle
- Botulinum Toxin (Botox®) injection: Botox temporarily paralyses the muscle fibres in the CP, and possibly also effects the sensory nerve fibres, allowing better relaxation and stretching, and after 3 days, resumption of the burp reflex, and symptom resolution.
- Mechanical Dilation (Balloon): This is performed through the mouth (endoscopically), and usually requires a general anaesthetic.
- The balloon is placed through the region of the CP muscle and inflated causing stretch, and breakdown of scar fibres within the CP muscle.
- This may be performed by your surgeon on the initial treatment, or subsequent treatments if required.
- Again, treatments can be repeated. SEE Fig.3
- Partial Cutting of the CP Muscle (CP Myotomy): This operation is most commonly performed through the mouth (endoscopic myotomy), without any cuts in the neck , though sometimes the muscle is approached through a cut in the neck (open myotomy). Most surgeons employ a Laser to perform the cut. The aim is to divide approximately 80% of the full thickness of the muscle, leaving 20% of fibres intact. The risk for complication is higher than for botox® or balloon, however It is generally a very effective treatment option, for refractory or recurrent cases.
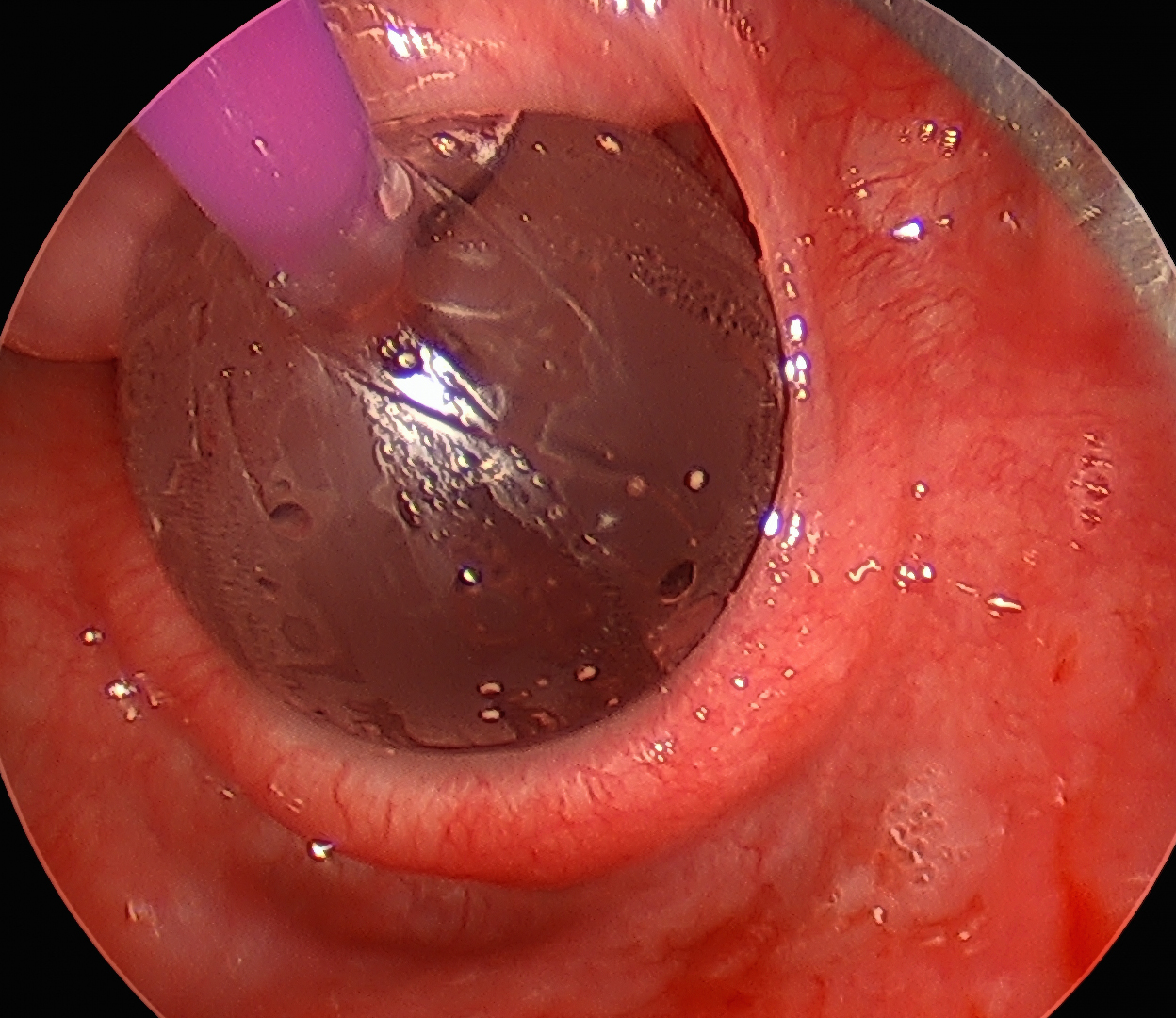
Fig. 2 – Balloon dilation across CP muscle
- Diet and lifestyle modifications to improve / initiate burping:
- Carbonated beverages
- Movement
- Gas-promoting foods
- Antacids
- Swallowing air
- See our separate information sheet on methods to promote burping
Treatment Outcomes:
85-99.5% of patients who undergo Botox® Treatment for R-CPD will have symptom relief, of at least the key symptoms, if not all the symptoms listed above.
75-80% of patients will have long-term relief – i.e. will not require repeat treatments.
For the 20-25% of patients who eventually have recurrent symptoms, repeat treatments can offer the same dose of botox® endoscopically, or a lower dose as an office-based EMG-guided percutaneous injection.
The addition of Balloon dilation may also be offered for revision procedures.
Partial CP myotomy may be offered for second revisions, or refractory cases.
What complications can happen?
The healthcare team will try to make the procedure as safe as possible but complications can happen. You should ask your doctor if there is anything you do not understand. Any numbers which relate to risk are from studies of people who have had this operation. Your doctor may be able to tell you if the risk of a complication is higher or lower for you.
Generally speaking, Botox® injection to the CP muscle, +/- Balloon dilation is a very safe and well tolerated procedure, and patients usually go home the same day as surgery on a normal diet, and with no pain, and no altered voice or breathing.
Possible Complications include :
- Complications of Anaesthesia
- As this procedure is performed under the care of an anaesthetist, your anaesthetist will be able to talk to you about these risks in detail, however it is a relatively short, low risk procedure. Care is taken to protect your pressure points.
- General Complications of any operation
- Pain: Most patients do not experience significant pain during or after this procedure. However, there may be some nose & throat discomfort which will improve over a few days. Simple over the counter pain relievers should be adequate. Occasionally, patients experience a dull earache during injections into the vocal fold itself, which is generally short-lived.
- Bleeding: There may be minor at the injection site in the CP muscle, but this is usually swallowed asymptomatically without any obvious blood from the mouth or in the mucous.
- Infection: The chance of infection is very low.
- Specific Complications of this operation
- mild Dysphagia (‘Slow’ Swallow): whilst the partial weakening of the CP muscle which commences approximately 3 days post-surgery is the desired effect leading to an ability to burp etc., this weakening also has the potential side effect of a slightly impaired swallow usually for denser solid foods such as meats, dense breads and hard vegetables. This occurs in approximately 30-50% of patients, is self-limited, and usually resolves within 2 weeks at most, but can be disconcerting. We advise a softer diet during this period, and avoiding those harder to swallow meats and breads until these symptoms have resolved.
- Reflux: For the same reason that a ‘slow swallow’ can occur early in the post-operative period, so too, patients may experience some reflux or even regurgitation of foods in the first couple weeks. This is due to the weakened CP muscle not being able to perform its reflex protective tightening when reflux in the oesophagus occurs. This is self-limited, and usually easily managed with simple diet and lifestyle changes such as smaller meals, greater time between meals and lying down, and simple use of barrier agents such as Gaviscon® dual action after meals. It is rarely severe, and always self-limited. Your doctor may occasionally prescribe an anti-reflux medication after your procedure to help limit these symptoms.
- Breathing problems: occur very rarely (<1%), and are usually due to some of the injected botox® seeping into the muscles of vocal cord movement which sit in front of the CP muscle. It is more common after the percutaneous injection approach than the endoscopic approach. If this happens patients may notice some noisy breathing or difficulty breathing a few days after the surgery when the botox starts to work. Whilst always self-resolving and usually not requiring any specific intervention, you should immediately notify your healthcare team, and if significantly concerned, You should immediately call 000 or attend the nearest Emergency Department. Similarly, any breathing difficulty in the first 24-48 hours after surgery is not normal and should be reported to your healthcare team.
- Minor damage to teeth/lips/gums: As with every microlaryngoscopy and/or oesophagoscopy where a rigid metallic telescope is placed into your throat through your mouth, there is a very small chance (<0.5%) of minor damage to teeth (chipped tooth or loosening), lips (abrasion or split lip) or gums (abrasion or bruising). Every precaution is taken to minimise this risk, including gentle tissue handling and protective mouthguards, but there is a small chance of damage, which if soft tissue, will heal spontaneously, and if dental, may require formal dentist assessment and restoration.
- Altered Tongue movement, taste or sensation: Anytime that an instrument is placed into the throat (larynx or oesophagus), there is a variable degree of pressure that is placed on the tongue. The degree of pressure depends on a number of factors such as the ease or difficulty the surgeon has in placing the scope (due to anatomical factors such as jaw opening, tongue and teeth size etc), and the duration of the operation (relatively brief for this surgery). It is uncommon but you may wake up with an altered taste (g. Metallic), or altered tongue sensation, and very rarely, altered movement of the tongue (e.g. slightly altered speech or chewing). This is due to pressure on the nerves of the tongue. It is almost always self-limited as the nerves recover, but can last for a few weeks, and can be annoying / disconcerting to experience.
- Oesophageal tear or perforation: Anytime that an instrument is placed into the oesophagus, such as with an oesophagoscopy, there is a very small chance (<0.1%) of a tear or small hole in the wall of the oesophagus. Whilst very rare, and almost always noticed at the time that it occurs, it can be a serious complication leading to inflammation of the chest contents around the heart and lungs, and will require a prolonged stay in hospital, feeding through a tube, and sometimes open surgery to repair. Untreated it can result in death, but as mentioned, it is an extremely rare occurrence.